
From April 23-26, the 35th annual Canadian Association of HIV Research (CAHR) conference was held in Winnipeg, Manitoba, “Under open skies: Rising to meet unprecedented challenges in the HIV response.”
Hundreds of conference attendees, including people living with HIV, community-based organizations, researchers, academics and allies from across the country gathered for Canada’s premier HIV-focused event that features four streams of keynote addresses, oral and poster presentations and ancillary events; Basic Sciences, Clinical Sciences, Epidemiology & Public Health Sciences, and Social Sciences.
PAN Presents at CAHR
PAN was thrilled to present three poster presentations at this year’s conference to acknowledge some of our incredible work over the last year. (click on poster images to enlarge)
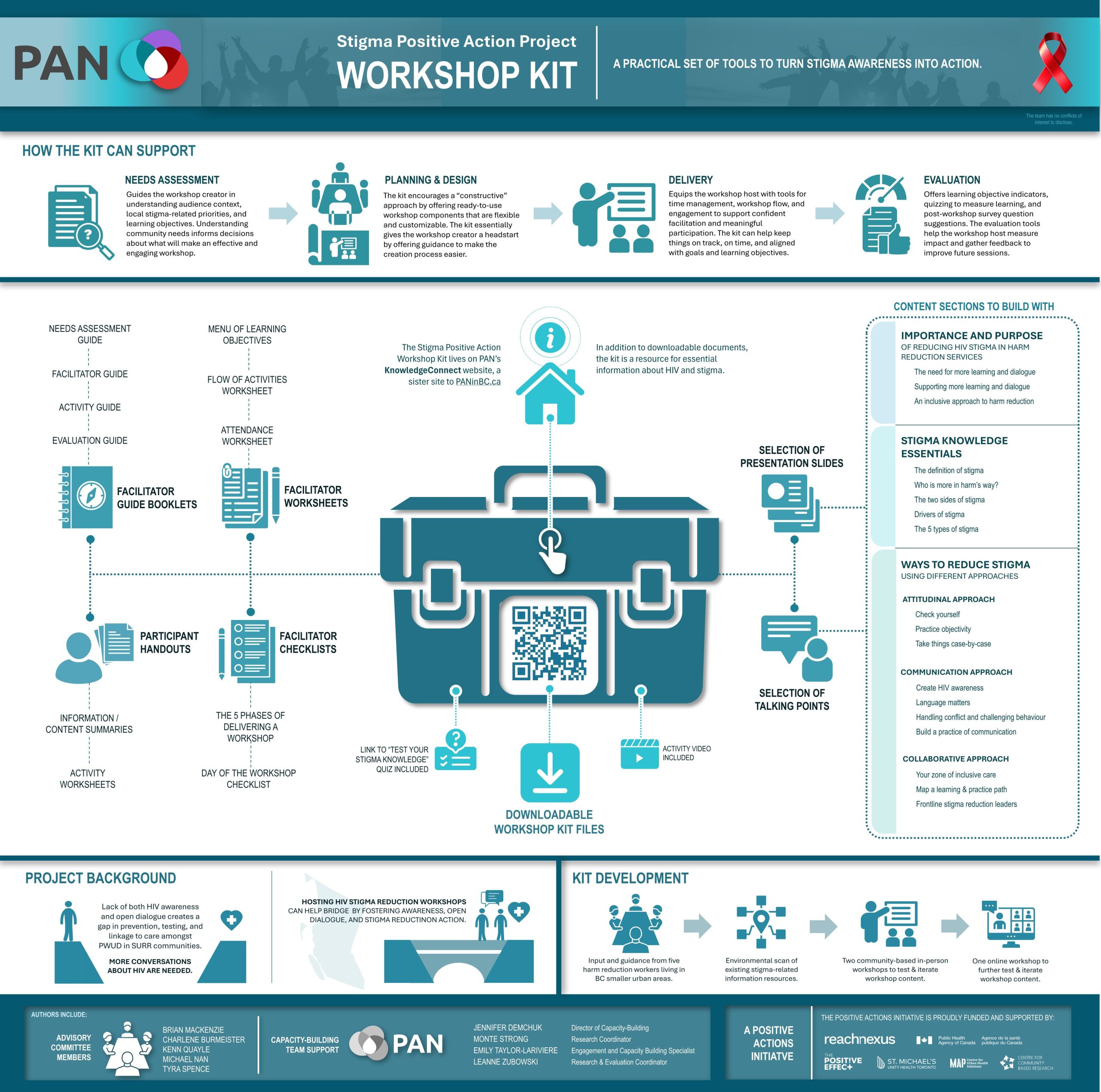
Stigma Positive Action Workshop ToolKit
The SPA Workshop Toolkit aims to support learning and promote dialogue about HIV and stigma in settings including outreach, support groups, harm reduction care delivery and stigma reduction workshops. It offers a series of modules that provides information to support dialogue, encourages reflection, and a variety of downloadable resource documents. The Toolkit is available for free on PAN’s Knowledge Connect learning portal website.
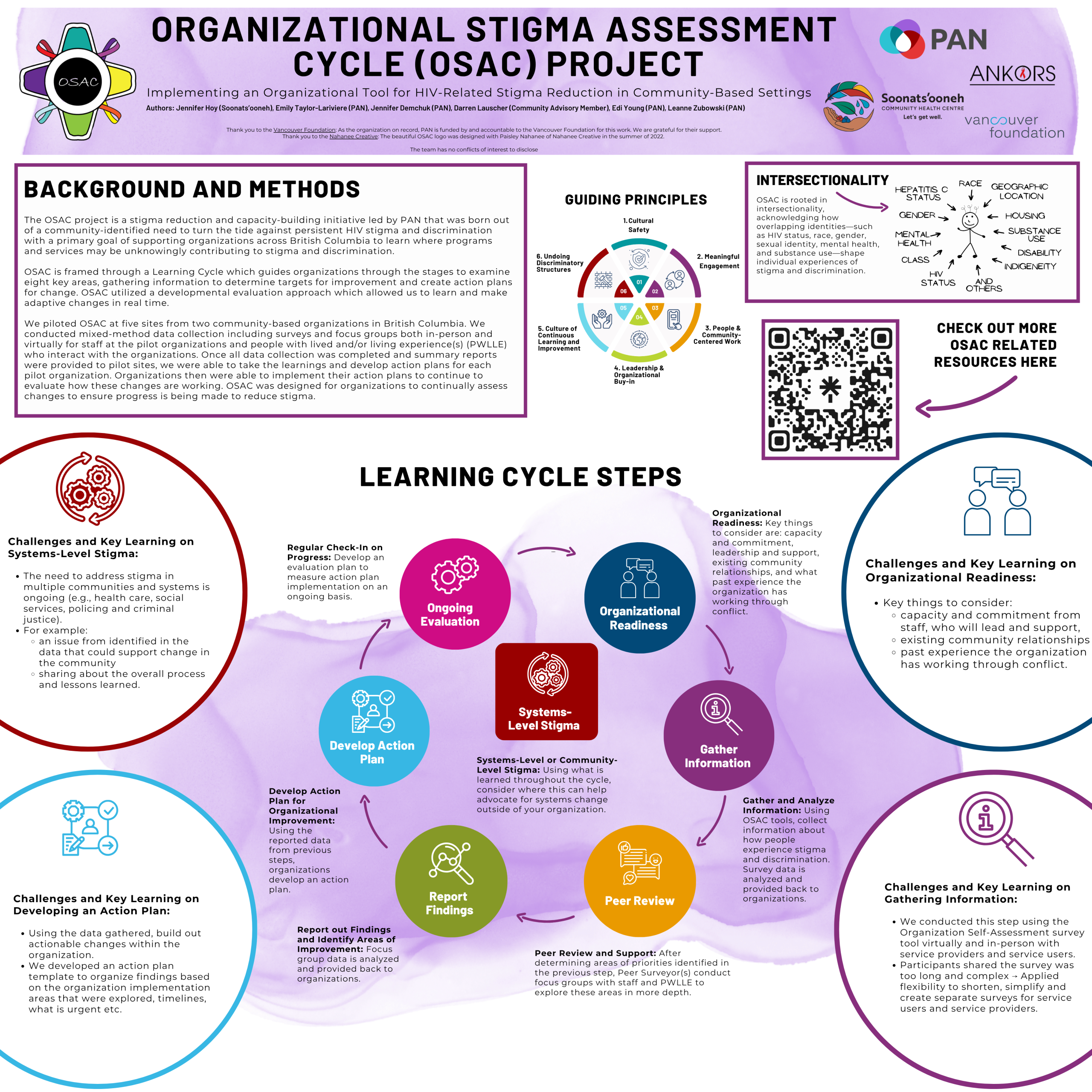
Organizational Stigma Assessment Cycle (OSAC) Project
The PAN team continues working to enhance stigma reduction through the launce of the Organizational Stigma Assessment Cycle project (OSAC), a combination of evaluation and capacity-building in a multi-step process to support organizations to learn where stigma and discrimination may inadvertently occur in their services. Using the learning from the initial analyses, capacity building will help organizations to identify target areas for improvement, and create action plans for change. The learning cycle will continue with regular evaluation of progress on targets, and assessment of further growth opportunities. Organizations may work through the process once or multiple times, depending on their organizational capacity.
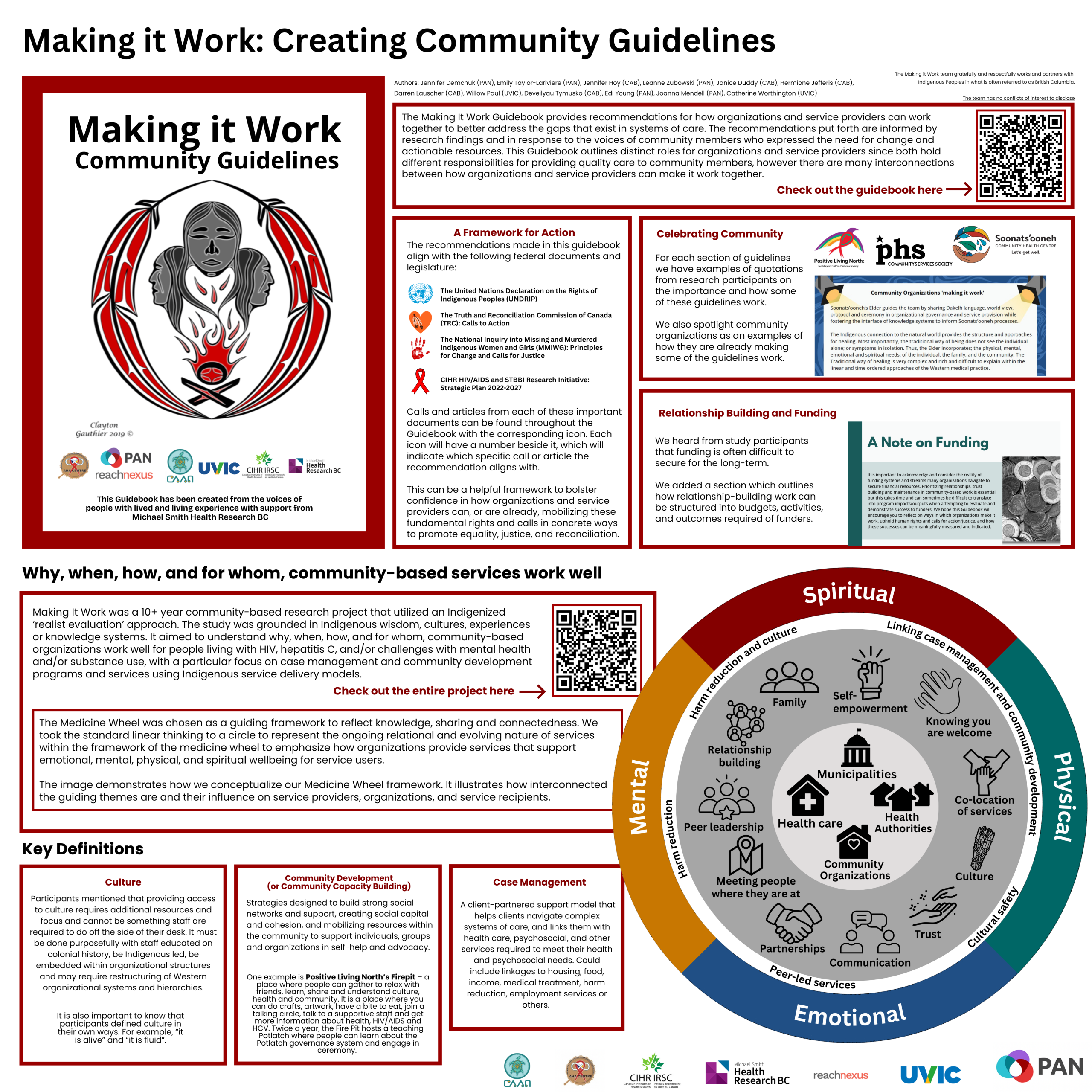
Making it Work (MIW) Guidebook Project
Making it Work was born out of conversations within the community when looking at the challenges people living with HIV, hepatitis C and other associated social and health issues face every day. The Making it Work Community Guidelines were developed and a subsequent Guidebook was produced that serves to share the knowledge from the Making it Work learnings and assist community-based organizations to bring that expertise to practice.
The Guidebook is intended to share the knowledge given by participants for organizations and service delivery; shares how to ‘make it work’, in terms of themes discovered from the study; and provide an actionable resource for organizations and service providers.
Throughout the Guidebook information is shared from PWLLE through guiding themes, organizational spotlights, and resources organized in terms of learning, training, and participation. The guidelines are interconnected and therefore user friendly to incorporate into organizations and service delivery.
Highlights from Throughout the Conference

Understanding and Acting for the Sidelined 2%: A Shared Language and a National Call to Care– presented by the Dr. Peter Centre
The first CAHR ancillary event for the week focused on a new series of resources. The “sidelined 2% lens” is a framework for designing and evaluating services by centering those most often excluded, rather than building systems around averages or mandates. It asks whether programs would truly work for people with complex, overlapping realities, including trauma, unstable housing, or substance use, and challenges organizations to adapt when the answer is no. By making invisible needs visible, this approach shifts focus toward real-life experiences and ensures services are built with, not just for, those most marginalized.
Applied in practice, the lens helps frontline teams identify who is missing from their reach and adjust outreach and trust-building accordingly, while guiding executives to advocate for flexible, wraparound funding that reflects whole-person needs. For policymakers, it calls for rethinking success metrics and designing systems “for the edges first,” recognizing that equity is achieved when those most sidelined are intentionally included from the start.
More information about Stitch In can be found here.
Canadian AIDS Society (CAS) Ancillary Event: Building Culturally Safe and Stigma Free Outreach
It was very exciting for the PAN team to learn more about the upcoming launch of the HIV Connect Program that has been in development for the last three years. At the very core, HIV Connect is a peer support strategy – PLHIV bring essential knowledge and insight to this work and were fundamental in the co-development of the content. Persistent stigma across systems that people are required to navigate every single day, workforce gaps in supporting peer engagement, and the need for culturally safe and trauma-informed outreach are essential. HIV Connect will be delivered through online, accessible learning modules that are designed to support anyone who works with PLHIV.
Ancillary Event – Middle Eastern and North African Trans and Gender Diverse Photovoice Art Exhibit: Stories of Resilience & Be/Longing – YSMENA Program
YSMENA was the first CBR program in Canada to center the voices of diaspora Middle Eastern and North African (MENA) youth in Canada. Their work focuses on promoting health, resilience and well-being of MENA youth populations across Canada through the documentation and interpretation of their lived realities through photography, journalling, and critical reflection. The participatory research design included three cohorts with 26 trans and gender diverse MENA newcomer youth in Toronto and Windsor. Initially considered youth to be 18-29 but extended to 39 after hearing from community that trans and gender diverse people often come out later and still identify as youth up to 39 years.
The ancillary event focused on the YSMENA CIHR Funded Trans Photovoice project, and featured the “Middle Eastern and North African Trans Photovoice Art Exhibit: Stories of Resilience & Be/Longing,” including a documentary and original artwork created by the youth during their time with the program.
Ancillary Event – Bots, Bias and Better Questions: Community-Based Perspectives on AI in HIV Research
This session explored the growing role of Artificial Intelligence (AI) in community-based research (CBR), particularly within HIV-related work, focusing not on judging its morality but on understanding its implications. Panelists including Bernice Thompson, Raymond Helkio, Dr. Rusty Souleymanov, and Ben Klassen, highlighted how concerns about bot activity compromising survey data quality initially sparked broader conversations about AI’s influence in research. A key issue discussed was that HIV-related data is deeply sensitive and non-neutral, meaning disruptions like bots or the use of AI tools can significantly affect data integrity and trust. The panel emphasized guiding principles such as GIPA/MIPA, shared power, plain language, and confidentiality, while raising critical ethical questions about AI’s use in data analysis versus tasks like literature reviews. They also explored both proactive and responsive approaches to AI integration, stressing the importance of transparency, informed consent, and community governance, particularly in disclosing when participant data may interact with third-party AI systems. Ultimately, the discussion underscored the need to involve community members in decisions about how their data is used, ensuring that AI adoption in CBR remains trust-based, ethical, and aligned with community expectations
Special Session: Setting the Context on HIV in Manitoba
This session highlighted how rising HIV rates in Manitoba reflect systemic failures rather than a lack of knowledge or tools, emphasizing that the issue lies in weak implementation and accountability across the health system. Speakers pointed to jurisdictional gaps between federal and provincial governments around Indigenous health, as a core barrier where responsibilities for testing, prevention, and care are defined but not effectively operationalized. HIV testing, framed as a clinical intervention, is too often treated as optional, limiting opportunities for early intervention and upstream prevention. With only about 68% of people living with HIV in Manitoba achieving viral suppression and projections suggesting cases could double, the data signals structural inequities rather than capacity issues. The discussion underscored how HIV exposes broader health system shortcomings that fail to serve Indigenous communities, especially in First Nations contexts where overlapping responsibilities lack coordination and accountability.
Panelists and community voices further illustrated how these systemic gaps play out on the ground, particularly in remote and underserved First Nations communities facing geographic barriers, workforce strain, stigma, houselessness, and substance use challenges. Health providers described an overburdened system focused on urgent care at the expense of prevention and public health, contributing to worsening outcomes, including prenatal risks and ongoing transmission. Community-led efforts including increasing education, expanding opioid agonist therapy, and advocating for culturally grounded care all highlight both resilience and urgent need. There was strong consensus that an effective response must be Indigenous-led, inclusive of First Nations, Métis, and Inuit perspectives, and supported by equitable funding, improved access to testing and care across regions, and meaningful collaboration between governments. Emerging initiatives, including a First Nations HIV strategy and calls for coordinated provincial and federal action, reflect growing momentum toward a more accountable, community-driven response.
“So Close Yet So Far; A Story of Australia and Canada and Their Respective HIV Responses and Outcomes for Indigenous Peoples” – Professor James Ward
Plenary Session; Epidemiology and Public Health
Over the past 40 years, Canada and Australia have experienced parallel HIV epidemics shaped by similar colonial histories, intergenerational trauma, and stark urban–rural health inequities affecting Indigenous populations. Despite these shared contexts, the outcomes diverge significantly. Canada continues to see a disproportionately high burden of HIV among Indigenous people (around 23% of cases compared to 3% in Australia), with earlier and more sustained impacts throughout the epidemic. Australia, by contrast, maintained relatively low HIV rates for decades through early, coordinated action—though recent years have seen concerning increases, particularly linked to injection drug use and shifting social dynamics.
Australia’s response has been defined by early implementation of surveillance systems, strong bipartisan support for harm reduction (including needle and syringe programs), rapid adoption of treatment and prevention tools (HAART, TasP, PrEP), and sustained national strategies. Community leadership including gay men and later Aboriginal and Torres Strait Islander communities, have been central, alongside culturally tailored campaigns and resources. Canada, while a leader in Indigenous data sovereignty and showing some progress, has struggled to achieve similar outcomes at scale. Across both countries, the evidence points to a clear lesson: biomedical advances alone are not enough. Effective responses require coordinated, multi-level interventions, sustained investment, and genuine implementation of equity, particularly for Indigenous communities disproportionately affected by HIV and other STBBIs.
“HIV Prevention – No Time to Lose” – Dr. Linda-Gail Bekker
Plenary Session – Clinical Sciences
Dr. Linda-Gail Bekker’s plenary emphasized both remarkable progress and urgent gaps in global HIV prevention. Despite decades of innovation, the world missed key 2020 targets, and by 2024 there were still 1.3 million new infections, half of which are among adolescent girls and young women in sub-Saharan Africa, and the rest among priority populations globally. Advances in antiretroviral therapy (ART) have transformed prevention, with nearly 50,000 trial participants demonstrating that treatment can also prevent transmission. New biomedical tools are expanding rapidly, including vaginal rings and long-acting injectable PrEP options like lenacapavir (LEN), a six-month injection showing strong safety and effectiveness across diverse populations, including young people and pregnant women.
Bekker highlighted the growing importance of choice in prevention. Studies like ALIGN show that when young people are offered multiple options (i.e. pills, injections, or rings), they can confidently choose what fits their lives, leading to better uptake and persistence. Combining primary and secondary prevention, alongside harm reduction strategies for people who inject drugs, strengthens outcomes across the HIV cascade. However, global momentum is threatened by political and financial instability, with many countries still reliant on donor funding and warnings from UNAIDS that progress could regress to early-2000s levels.
The path forward requires scaling up access, reducing costs, and normalizing prevention. Bekker called for bold action: accelerating PrEP uptake, expanding access to innovations like LEN (with hopes of lower-cost generics), and creating demand by embedding services in communities. Programs that integrate HIV prevention into everyday setting like fast, accessible clinics or community-based initiatives, demonstrate how delivery models must evolve beyond traditional healthcare systems. At the same time, she stressed that stigma remains a major barrier without a biomedical solution, making community leadership and engagement essential.
Ultimately, Bekker framed this as a moment of both urgency and opportunity. Ending HIV will require more than biomedical advances, it demands rethinking global health approaches, centering social determinants, and meeting people where they are. Her closing message was clear: prevention must be scaled, democratized, and community-driven. Without bold, coordinated action now, the global response risks falling behind—but with it, a prevention “revolution” remains within reach.
Social Sciences Plenary Session – Dr. Notisha Massaquoi – From Dialogue to Action: Reimagining Black HIV Equity Research in Canada
Dr. Notisha Massaquoi’s presentation framed HIV health equity for Black communities in Canada as both a research and systems failure, but also an opportunity for transformation. Drawing on the Silent Voices of the HIV/AIDS Epidemic study, she highlighted how inconsistent race-based data collection and decades of disparity-focused research have normalized inequities rather than resolved them. While we understand where gaps exist, far less progress has been made in developing solutions that are meaningful, effective, and grounded in Black community realities.
Massaquoi argued that achieving equity requires a fundamental shift in how research is designed and conducted. Instead of beginning with deficits, research must start from the lived experience, expertise, and leadership of Black communities. The Kona Project exemplifies this shift, bringing together researchers, community organizations, and institutions to co-create a shared research agenda. Built over 18 months through trust-based engagement, Kona demonstrates that when communities are positioned as equal partners and knowledge holders, research becomes more relevant, accountable, and action-oriented. This approach is grounded in ten core values, including accountability, reciprocity, collective power, and the idea that data can either reinforce oppression or serve as a tool for liberation.
Importantly, the presentation moved beyond theory to practice. A key takeaway was that equitable research must translate into accessible, culturally grounded services; “we are calling for a future where equity is not an aspiration but a non-negotiable outcome of our collective work we conduct together.” Through TAIBU Community Health Centre, the development of the AYA Circle of Care demonstrates how community-led models can close service gaps. In a region like the Greater Toronto Area where HIV rates are high but tailored services have been scarce, this program provides holistic, family-centered care for Black communities. Early outcomes, including supporting a pregnant newcomer and the birth of an HIV-negative child, illustrate how trust-based, culturally relevant care can directly improve health outcomes.
Overall, Massaquoi’s message was clear: advancing HIV equity in Canada requires a paradigm shift from studying disparities to building solutions with communities. This means rethinking power, investing in community leadership, and embedding equity into both research and service delivery. Without this shift, inequities will persist; with it, there is a pathway toward meaningful, sustained change in HIV outcomes for Black communities. There is no HIV-agenda in Canada that can be moved forward without the inclusion of Black and Indigenous people.
HIV Sustained Remission and Possible Cure: A Lake Breaker Abstract Presentation
Sharon Walmsley – University Health Network
At a special abstract presentation, Sharon Walmsley presented a landmark Canadian “first” in HIV cure research through the case of the “Toronto patient.” This individual, living with HIV for over two decades and choosing to remain anonymous, underwent a bone marrow transplant to treat acute leukemia using donor stem cells carrying the rare CCR5-delta-32 mutation, which prevents HIV from entering immune cells. Following the transplant, the patient stopped antiretroviral therapy in mid-2025 and, as of early 2026, has maintained undetectable HIV levels with no measurable viral activity, representing sustained remission and a possible cure.
Walmsley’s presentation emphasized both the scientific significance and the limitations of this breakthrough. The “Toronto patient” is now among a very small number of individuals, 10 globally, to achieve long-term HIV remission through this approach, reinforcing that a cure is biologically possible. However, she underscored that bone marrow transplants remain too risky and complex to be used broadly, as they are only appropriate in cases where patients already require treatment for life-threatening cancers. Instead, the case provides critical insights into HIV eradication strategies, with specific attention to targeting viral reservoirs, and serves as a proof-of-concept guiding future, more scalable cure research.
More resources can be found here:
University Health Network: Canadian First: Man Living with HIV in ‘Sustained Remission’ After Bone Marrow Transplant
University of Toronto: Toronto team leads first-in-Canada case of sustained HIV remission
AIDSMAP: Toronto man cured of HIV after stem cell transplant
Global News: Toronto man’s HIV in remission after bone marrow transplant to treat cancer
Globe and Mail (paywall): Toronto man poised to become the first Canadian cured of HIV
Village Report: Toronto man’s HIV no longer detectable after bone marrow transplant
Special Session – Communities in Action: Showcasing Canada’s New HIV/AIDS and STBBI Community-Based Research Investments

Hosted by the Canadian Institutes of Health Research (CIHR), newly funded teams from the Team Grant: HIV/AIDS and STBBI Community-Based Research (CBR) competition that has committed to $23-million in 19 community-based research teams across the country.
 As a successful recipient of Community-Based Research (CBR) Team grant funding, PAN’s Joanna Mendell presented the Thrive project to conference attendees. Over the past five years, PAN has convened people with lived and living experience, community-based organizations, researchers, and partners from health authorities and public health to identify research priorities for smaller urban, rural, and remote (SURR) communities across BC. With this funding, the team will now bring these priorities to life over the next five years. Thrive brings together an engaged network of peers and partners focused on advancing STBBI health equity for people who use drugs and/or have experienced incarceration. The team will meet regularly to support collaboration, capacity building, and project oversight. Key activities include hosting a community of practice, mapping STBBI services across BC, highlighting community-led models of care, and funding local groups to implement and evaluate STBBI interventions using a community-led implementation science approach. You can read more about the Thrive project here.
As a successful recipient of Community-Based Research (CBR) Team grant funding, PAN’s Joanna Mendell presented the Thrive project to conference attendees. Over the past five years, PAN has convened people with lived and living experience, community-based organizations, researchers, and partners from health authorities and public health to identify research priorities for smaller urban, rural, and remote (SURR) communities across BC. With this funding, the team will now bring these priorities to life over the next five years. Thrive brings together an engaged network of peers and partners focused on advancing STBBI health equity for people who use drugs and/or have experienced incarceration. The team will meet regularly to support collaboration, capacity building, and project oversight. Key activities include hosting a community of practice, mapping STBBI services across BC, highlighting community-led models of care, and funding local groups to implement and evaluate STBBI interventions using a community-led implementation science approach. You can read more about the Thrive project here.
This CAHR session was a great opportunity to hear from 12 of the funded projects that are all working in different ways to strengthen community-based research and the response to STBBIs in communities around the country.
Special Session – Decentralized STBBI Testing: Empowering Communities and Expanding Access
This panel offered a strong overview of practical options for delivering STBBI testing outside traditional clinical settings. Speakers highlighted dried blood spot (DBS) testing as a long-standing, accessible method that uses a simple finger prick rather than a venous blood draw, making it easier to implement in community settings. While DBS can improve reach, it involves extended turnaround times and may risk of loss to follow-up. In contrast, point-of-care options, such as rapid tests that give results within minutes and on-site molecular testing that can confirm infections, can support same-day screening, diagnosis, and linkage to care, helping reduce those gaps.
Dr. Catherine Card from the National STBBI Laboratories at the National Microbiology Laboratory shared over a decade of success with the DBS program, which has consistently identified higher positivity rates than traditional lab testing, suggesting it is reaching priority populations. A national DBS training program is also available, including videos, manuals, and evaluation tools. (accessed via: [email protected])
Tracy Taylor discussed the broader landscape of community-based testing, including DBS, rapid antibody testing, and confirmatory molecular testing using technology like the Cepheid GeneXpert machine. These technologies are approved in Canada for hepatitis C diagnostic, and HIV viral load testing, and offer important opportunities to expand timely, decentralized care.
Finally, Veda Koncan shared a successful community testing event in Swan River, Manitoba, led by the Manitoba Harm Reduction Network. By bringing together health and social service providers, the team was able to test for hepatitis C and link people to care on the same day, demonstrating a collaborative, community-led model that is now being shared for others to adapt.
More information about all of the CAHR abstracts, sessions, and content can be found here.